
THE MARICOPA HEALTH CARE INTEGRATED EDUCATIONAL SYSTEM (HCIES):
A Collaborative Model for Surviving Health Care Change
A Collaborative Model for Surviving Health Care Change
by
Mary F. Briden, M.A., CLS (NCA)
Director, Transfer Education and Special Projects
Maricopa County Community College District - Tempe, Arizona
Mary F. Briden, M.A., CLS (NCA)
Director, Transfer Education and Special Projects
Maricopa County Community College District - Tempe, Arizona
"The dogmas of the quiet past will not work in the turbulent future. As our cause is new, so must we think and act anew."
-Abraham Lincoln
Executive Summary
Recognizing the need for Arizona’s health care professionals to possess different skills, attitudes, and values, the Maricopa County Community College District (MCCCD) was compelled to make a critical decision regarding health care education. To respond to the dramatic changes occurring in health care delivery, the MCCCD created the Maricopa Commission on Health Care Education Reform (HCER). The Maricopa Health Care Integrated Educational System (HCIES), which grew out of the combined efforts of health care stakeholders, is a systems model driven by the impact of its products and services. The major components of this systems model are Input, Process, Outcomes, and Impact. The HCIES strives to meet the community’s health care needs via the development of a skilled and flexible workforceone that acknowledges and respects the realities of shared scopes of practice. Its strong relationships and partnerships among the various health professions, education programs, accreditation and regulatory boards, and the health care community make the HCIES especially unique. Although the HCIES model was developed in response to the tremendous changes in the health care delivery system, it transcends health care and can be easily applied to other professions.
Introduction
Arizona is at the forefront of the dramatically changing health care environment. Ranking fourth in the nation for managed care participation, Arizona has experienced many shifts that other states are only beginning to face. As a result, the delivery of care has moved markedly toward the home and community and away from the hospital environment. However, the institutions that educate and regulate the professions and occupations providing care remain entrenched in a health care world of yesterday. The outcome is an immobilized workforce, unable to adapt to a rapidly, continually reforming health care delivery system. Ultimately, this is felt most by those very persons requiring the care and support of the workforce-the patients. It became evident in 1993 that the Maricopa County Community College District (MCCCD) was in the throes of the evolving managed care movement. Its various health occupation programs (37 allied health and 5 associate degree nursing programs) began to experience a decrease in available job opportunities for program graduates. This downhill slide continued, until in 1995, approximately 50 percent of nursing graduates were not employed directly upon graduation, and the number of allied health and nursing clinical rotation sites had disappeared in somewhat similar proportions. Employers clearly stated that MCCCD was producing too many graduates in areas no longer being utilized, and not enough in areas of need. The new employment needs were tied directly to the emergence of multi-skilled and multi-competent health care workers, who could function comfortably in nonlinear environments where, unlike the past, equilibrium is rare and control is counterproductive. Clearly, the issue facing Maricopa was shared scopes of practice-a statement of heresy in the past, but a reality for the present and foreseeable future. Not to change would have been the riskiest practice. How does an educational system like Maricopa continue to provide the community with a skilled health care workforce that meets employer and consumer needs during the most radical change our health care delivery system has ever experienced? As a first step, the MCCCD created the Maricopa Commission on Health Care Education Reform (HCER). The Commission was charged with the development, initiation, implementation, and evaluation of MCCCD’s educational response to the dramatic changes taking place in health care. The most difficult challenge was to develop a workforce that could adapt and evolve in sync with the transformation occurring in care, while performing cost effectively to protect and improve the public’s health. The Commission realized the approach to health care education reform would have to be carefully planned and coordinated for a coherent, efficient, and flexible model to be developed. Furthermore, the model would have to reflect a strong relationship among educational programs, the variety of settings where care is provided, the accreditation and regulatory agencies, and, of utmost importance, the local health care community in general. This dynamic health care reform initiative is unique in that the MCCCD and the Commission jointly determined allied health and nursing professional programs would have to be brought together. This coalition provided the unity and sharing of insights and experience necessary to create what is now called the Maricopa Health Care Integrated Educational System (HCIES).
MCCCD-Building on Existing Strengths
Despite the enormity of this reform initiative, Maricopa nonetheless believed it could undertake this incredible challenge. Maricopa’s success so far can be attributed in large part to its existing strengths, some of which follow:
- The nation’s second-largest multi-college system
- Largest single provider of higher education in Arizona (160,000 credit students and 30,000 non-credit/special interest students per year)
Largest provider of job training in Arizona - Graduates more than 2,000 individuals per year for the community’s health care workforce, constituting the largest single provider of health care workers in Arizona
- Ranks among the nation’s leading institutions of higher education in the use of computers and telecommunications
- 62 percent of Arizona State University’s (ASU) upper division enrollment comes from students with transfer credits earned from enrollment at one of ten Maricopa Community Colleges
- 50 percent of ASU’s undergraduate students have earned credits from one of the ten Maricopa Community Colleges
- 46 percent of ASU’s baccalaureate degrees are awarded to former MCCCD students
- Diverse student body represents the variety of ages, interests, backgrounds, and racial/ethnic mixture of the local population.
- 40 percent of all adults residing in Maricopa County have attended one of the Maricopa Community Colleges
- At least 9 percent of Maricopa County’s adult population attends a Maricopa Community College within an academic year
- Enjoys tremendous community support, as evidenced by the November 1994 Maricopa County voters’ approval of a $385.8 million capital development program to be paid with general obligation bonds
MCCCD Process and Response
In February 1995, MCCCD sponsored a Day of Dialogue focusing on changes in health care. Nursing and allied health faculty, as well as administrators and community representatives, gathered to discuss key issues in health care education and delivery systems. The keynote speaker representing the Pew Health Commission, as well as community leaders in health care, challenged the participants to examine the changes in health care at both the national and regional levels. As a follow up to the Day of Dialogue, a planning committee composed of nursing and allied health members was formed to explore the issue of change and its impact upon health care education programs in the Maricopa Community Colleges. In late May 1995, the planning committee began its work of collecting data on the changes in health care from a variety of perspectives and discipline all parties agree to the processs. This included meeting with leaders of the Pew Commission, attending national and regional conferences devoted to health care changes, conducting extensive literature searches, and interviewing many community health care leaders to better understand reform issues and their impact on health care education. The planning committee, using outcomes from their activities, next planned and sponsored the MCCCD Health Care Education Reform Summit on October 27, 1995. The summit disseminated information to nursing and allied health faculty, administrators, and community health care leaders, and elicited interest and participation in health care education reform issues affecting the Maricopa Community Colleges.
Following the summarized presentation of Summit outcomes and recommendations, the planning committee was officially dissolved and the Maricopa Commission on Health Care Education Reform (HCER) was created. Additionally, a Maricopa Health Care Education Reform Advisory Council was formed.
Commission and Advisory Council Structure
The HCER Commission was charged with the development, initiation, implementation, and evaluation of MCCCD’s educational response to the dramatic changes taking place in the health care arena. It is comprised of 16 members (7 community and 9 MCCCD), with leadership composed of three tri-chairs representing allied health, nursing, and the community. The Commission also directs five task forces, each co-chaired by a community representative and a MCCCD representative from the Commission.
Commission task force responsibilities are as follows:
Task Force 1 Forecasting and Modeling
Task Force 2 Competency Development
Task Force 3 Educational Pathways
Task Force 4 Resource and Organizational Development
Task Force 5 Evaluation and Assessment
The Advisory Council acts as a focus group to provide insight and direction to the Maricopa HCER Commission's initiatives. This council is comprised of influential members of the community who meet quarterly.
Commission Reports
In September 1996, the Initial Commission Report was submitted, which contained 45 recommendations. Among these were the initial development of a model depicting necessary provider skills across the continuum of care and the adoption of a comprehensive, integrated educational system for health care (including both allied health and nursing) within the MCCCD-called the Maricopa Health Care Integrated Educational System (HCIES). This integrated system provides entry level education, continuing education, and opportunities for professional renewal and re-training in a continuing collaboration with the community. All 45 recommendations were accepted by Maricopa administrative leadership.
In February 1997, an Interim Commission Report was submitted that included the newly developed HCIES as the overarching structure and process for the work of the Commission. The salient characteristic of the HCIES model is also the key to its effectiveness: it is driven by the impact of its products and services, and it reponds to the dynamic nature of the health care system in partnership with the local health care community. Sensitive to the realities of resources, this system will become a self-sustaining tool for evaluation, communication, and critical feedback. Furthermore, it reflects the need to encompass regional and other accreditation program requirements. The HCIES Mission Statement and Goals are found in Attachment A, and the HCIES Conceptual and Descriptive Models are depicted in Figures 1 and 2.
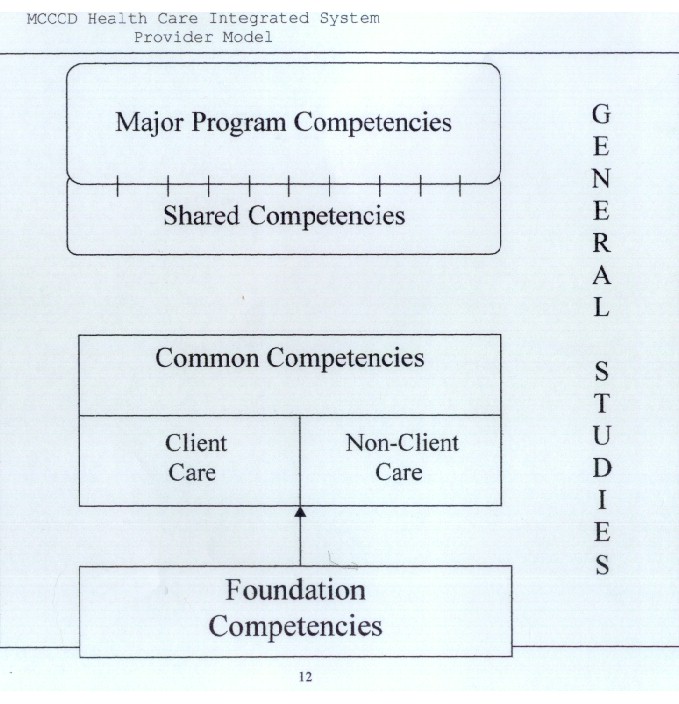
Also included in the report was a Health Care Provider Model encompassing both generalist and specialist health care education. This model is based on common core content (shared scope) that is competency driven, and, when once mastered, need not be repeated. The common core composed of Foundation, Common, and Shared Competencies will enable students to cross over to other disciplines to achieve additional skills and specialization competencies without backtracking. The Maricopa Provider Model-a work in process-and accompanying definitions are listed in Attachment B and Figure 3.
September 1997 is the date set for the Commission’s next interim report. It is scheduled to include the organizational model for the HCIES, draft models relating to Articulation and Assessment, the Foundation Competencies and corresponding course modules, and an outline of the HCIES Student Career Pathways.
Next Steps
Currently, the Commission is initiating the development of an Education and a Forecasting Model. A transition implementation plan is forthcoming that will include a component for faculty and staff development and cross-training. The established HCIES implementation date has been identified as Fall 1998.
Regulation of Health Care Professions
In support of Maricopa’s health care education reform initiative, two State Initiatives Support Grants have been awarded to the MCCCD by the University of California San Francisco, supported by The Pew Charitable Trusts. The initial grant had as its primary goal the continuation and expansion of the Maricopa dialogue on the reform of health care educational programs. The funding provided by the grant, together with MCCCD resources, were utilized to convene a second Summit on April 4, 1997-a direct result of the initial Commission task force recommendations for increased awareness and study of the impact of health care education and workforce reform on workforce regulation.
The April 4, 1997, Maricopa/Arizona Dialogue, entitled "Impact/Implications of Workforce Regulation on Plans for the Health Care Integrated Educational System," served as the initial convening of statewide representatives of Arizona stakeholders-community colleges, universities, health care providers, regulatory agencies, and interested legislators. The conference sponsored the authorship of four distinct white papers addressing specific questions on the HCIES’s effect on existing regulatory and accreditation requirements and standards. The white papers were authored and presented by medical radiography, clinical laboratory science, nursing, and physical therapy. The outcome of the conference demonstrated strong conceptual support for the MCCCD proposal of the HCIES as a comprehensive, integrated, educational systems model for health care education.
This Summit led to the creation of a statewide Task Force on Workforce Regulation as it relates to health care. The goals identified for the task force are twofold:
- To continue to expand the Maricopa dialogue on health care education reform cross Arizona by discussing the impact of health care workforce regulations on the HCIES
- To develop operational plans to change health care workforce regulations, as necessary, to allow for the implementation of the HCIES.
Invitation for membership on this statewide task force has been extended to accreditation, regulatory, and credentialing agencies; allied health and nursing professional organizations; educators; health care providers; community members; legislators, and legislative staff.
The second State Initiatives Support Grant, entitled "Arizona: Planning for Regulatory Changes Which Support the Proposed Health Care Integrated Educational System," follows up the April 1997 Summit. The intent is to analyze recommendations and policy options, including the political realities and cost implications of proposed regulatory reforms relating to the Maricopa HCIES.
Dialogue, Collaboration, and Partnership
In our ever-changing world, accreditation and regulatory boards, professional organizations, and the community must agree to work together to keep pace with the dramatic changes in the health care delivery system. Instead of formulating strategies to "preserve" their professions, they must assume a proactive approach to the issues at hand. The HCIES model can be used as a starting point to progress and survive-together. Although the HCIES model was developed in response to the tremendous changes in the health care delivery system, it transcends health care and can be easily applied to other professions.
The Maricopa Health Care Education Reform initiative will be accomplished through dialogue, collaboration, partnership, and trust among the various health professions across the state of Arizona, as well as nationally. Only together can professions drive legislative changes that respond to the integrated delivery system created by the coordination of health care services across providers, functions, activities, and settings. Only together can professions garner enough attention and support to continue to deliver safe, quality, and cost-effective health care to protect the consumers we serve. Maricopa welcomes your input and invites you to join with us in our quest to work together in mutual respect and partnership.
Additional information and updates are available via the Commission’s Web Site: http://www.dist.maricopa.edu/hcies/hcies9.htm.
References
Arizona Hospital and Healthcare Association, Education Foundation (1997). The Healthcare Institute at the Arizona Hospital and Healthcare Information Sheet. Phoenix: AHHA.
Cox, K.H., A. Wells, and C. Wheeler (1994). Institutional Responsiveness: A White Paper. National Network of Health Career Programs in Two-Year Colleges, Hurst, TX, April 15.
Maricopa County Community College District (1996). Initial Report. Maricopa Commission on Health Care Education Reform. Tempe: MCCCD.
Maricopa County Community College District (1997). February Interim Report. Maricopa Commission on Health Care Reform. Tempe: MCCCD.
Maricopa County Community College District (1997). The Maricopa/Arizona Dialogue: Impact/Implications of Workforce Regulation on Plans for the Health Care Integrated Educational Systems Final Report. San Francisco, CA: UCSF Center for the Health Professions, State Initiatives Program Regulatory Reform Grant.
National Council of State Boards of Nursing (1997). Emerging Issues: Accreditation/Approval of Nursing Education Programs. Chicago: NCSBN.
Pew Health Professions Commission (1991). Healthy America: Practitioners for 2005. San Francisco, CA: UCSF Center for the Health Professions.
Pew Health Professions Commission (1995). Critical Challenges: Revitalizing the Health Professions for the Twenty-First Century. San Francisco, CA: UCSF Center for the Health Professions.
Pyles, C.D. (1995). Call to Action: Community Colleges Preparing the Health Care Workforce for the 21st Century: An Abstract. National Network of Health Career Programs in Two-Year Colleges. Chicago, IL, September 28.
Attachment A
Maricopa Health Care Integrated Educational System (HCIES)
Mission Statement
The HCIES is a comprehensive and integrated system for health care education within the MCCCD. It is designed to respond to the dynamic and evolving nature of the health care system; it is focused on collaboration with the local health care community; and, it is sensitive to access for diverse populations. All programs and educational offerings within the HCIES emphasize the achievement of relevant competencies and ensure value to the individual, the employer, and the community.
Goals
- To provide Effective and Relevant education/training programs to meet the contemporary and emerging needs of the health care community.
- To provide a Coherent and integrated program of education and occupational training for health care.
- To provide health care curricula and programs which are Flexible, responsive, and accountable to the evolving nature of the health care system.
- To collaborate with the health care community to enhance the achievement and success of students and to facilitate their employment.
- To provide health care programs and training that promote quality of care and appropriate standards of practice and meet accreditation requirements.
- To develop, modify, and maintain current and relevant learning outcomes and educational competencies.
- To provide education/training programs that are accessible to diverse populations.
- To recruit, retain, and reward qualified faculty and support personnel who promote a standard of excellence and who reflect the diversity of the community.
- To provide Efficient policies and operations that promote self-correction and continuous improvement, maximize resources, prevent redundancies, and ensure structural integrity.
- To maintain and use current technology and equipment that support the standards of practice and the complex institutional needs required to offer health care education and training.
- To provide the education and training necessary for licensure and certification as may be required.
- To provide opportunities for re-careering and professional renewal consistent with the mission of the community colleges.
Attachment B
7/01/97
Provider Model
Definitions
Competency: Demonstrated psychomotor, cognitive and/or affective behavior
Levels of Learning:
Level I: (Foundation Competencies) Student with little or no experience in health care. Learns entry-level concepts that need to be acquired by all workers in health care settings. Emphasis is on awareness and basic skill development.
Characteristics:
- Understands rules/standards that govern behavior and practice in health care
- Uses basic definitions of terminology
- Understands basic job expectations and attitudes
- Performs simple procedures
- Aware of unique aspects of system/work environment
Level II: (Common Competencies) Continuing student. Learns core principles of client and/or non-client care. Emphasis is on performance of select skills and procedures and ability to effectively respond to simple problems.
Characteristics:
- Performs selected skills/procedures and understands their rationale
- Observes symptoms and acts appropriately
- Discriminates between normal and abnormal conditions and situations
- Follows established guidelines in the care of clients and/or in the management of health information/documentation
- Applies simple problem-solving techniques in addressing job-related issues and/or client care
- Understands and interacts within context of system/work/people
Level III: (Major Program/Shared Competencies) Students who have met all program prerequisites and accepted into a specific major. Emphasis is on application of theory and research to solve complex problems and situations. Develops action plans based on previous learning and analysis of problem.
Characteristics:
- Assesses and responds to different, varying and complex situations/problems
- Demonstrates mastery of standard concepts and skills related to major
- Anticipates situations/problems and determines appropriate action
- Integrates knowledge into practice
- Demonstrates leadership behaviors in system/work/people contexts
Figure 1
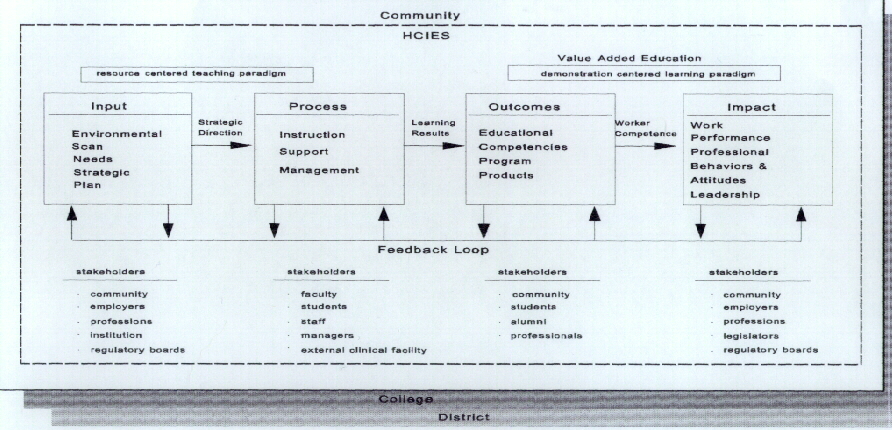
Figure 2
Figure 3
COPYRIGHT 2000. Rights to copy and distribute this publication are hereby granted to members of the Council on Licensure, Enforcement and Regulation (CLEAR), providing credit is given to CLEAR and copies are not distributed for profit.